

ACL Rehabilitation
Quadriceps Weakness After ACL Injury: Why It Happens, Why It Persists, And How To Restore It
The Quadriceps Problem At The Heart of ACL Rehabilitation
Ask any experienced ACL rehabilitation clinician to identify the single most consistent and clinically significant challenge across the rehabilitation process, and the answer is almost always the same: restoring the quadriceps.
Quadriceps weakness after ACL injury is not simply a matter of muscle being out of condition. It involves a complex interaction between joint pathology, neurological inhibition, surgical trauma, disuse atrophy, and the progressive loading demands of rehabilitation. It is one of the most researched topics in sports medicine and, despite that research, one of the most persistently mismanaged in clinical practice.
As Mick Hughes — one of the most widely respected ACL rehabilitation clinicians in contemporary practice — has consistently emphasised in his rehabilitation frameworks, quadriceps restoration is not a background consideration in ACL rehabilitation. It is the primary physical target that everything else is built around. You cannot progress running, plyometrics, or return to sport safely without first addressing it systematically and objectively.
Arthrogenic Muscle Inhibition: The Neurological Mechanism
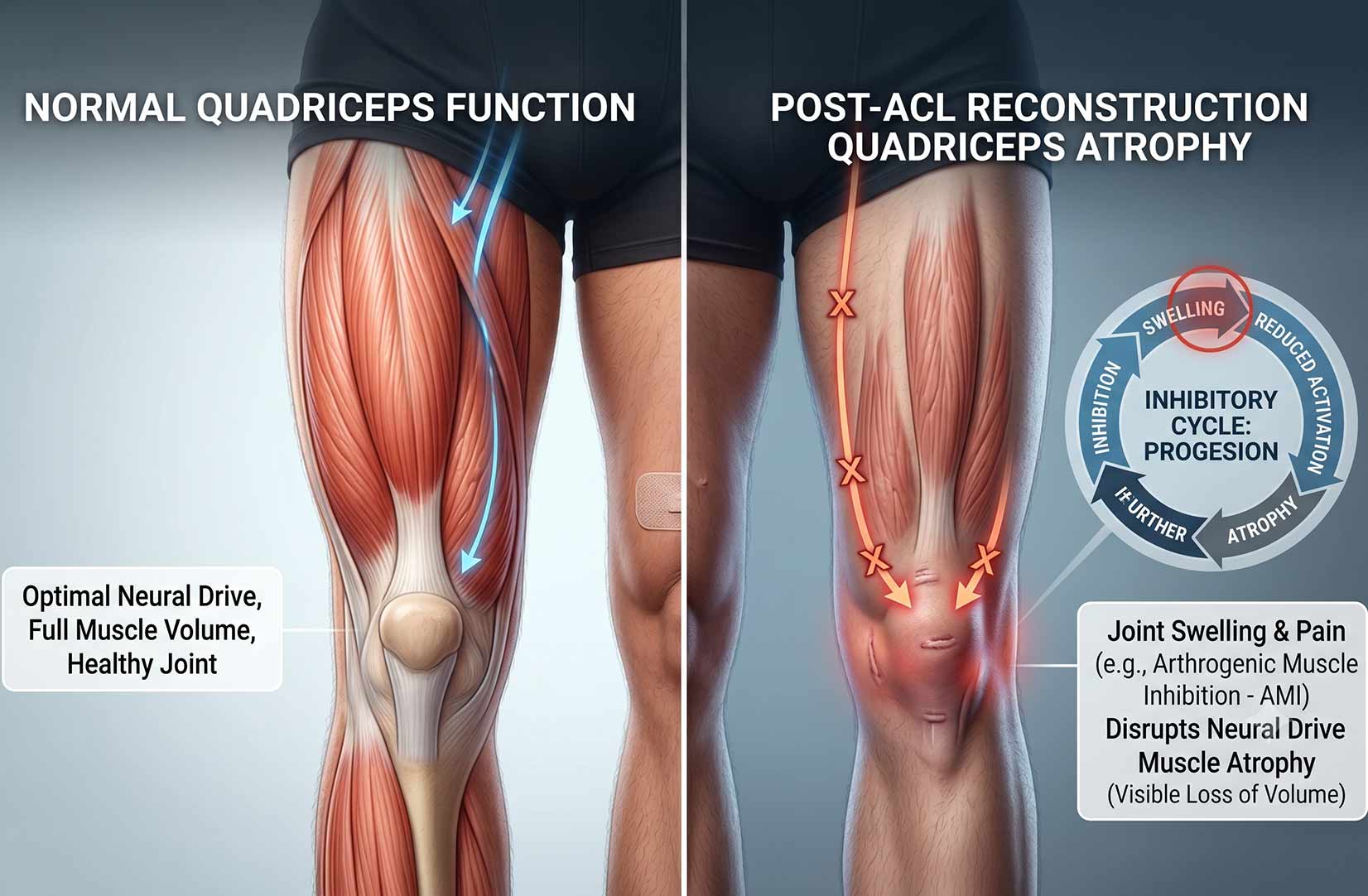
The most important concept in understanding quadriceps weakness after ACL injury is arthrogenic muscle inhibition — a neurological protective response in which swelling or pathology within the knee joint directly inhibits the motor neurone pool supplying the quadriceps muscle group.
This is not weakness in the conventional sense. The muscle fibres are present and structurally intact. The motor pathway is functional. But the nervous system, in response to afferent signals from mechanoreceptors and nociceptors within and around the joint, actively reduces its drive to the quadriceps. The result is a muscle that cannot produce its full force potential regardless of how hard the patient tries.
Rice and McNair (2014), in a highly influential review in Seminars in Arthritis and Rheumatism, documented the neurophysiology of arthrogenic muscle inhibition in detail — demonstrating that even relatively small volumes of intra-articular fluid, as low as 20 to 30 millilitres, are sufficient to significantly reduce quadriceps activation. The clinical implication is direct: swelling management is not simply about comfort or appearance. It is a prerequisite for meaningful quadriceps restoration.
Arthrogenic Muscle Inhibition
The mechanism in plain terms
When the knee joint is swollen or injured, sensory receptors within the joint capsule send inhibitory signals to the spinal cord that reduce motor neurone drive to the quadriceps. This is an involuntary neurological process. It cannot be overcome through effort or motivation alone. It requires targeted management of the underlying joint pathology combined with specific neuromuscular activation techniques to restore voluntary quadriceps drive.
Why Quadriceps Weakness Persists Long After Surgery
Lepley et al. (2017), writing in the Journal of Athletic Training, demonstrated that quadriceps strength deficits following ACL reconstruction can persist for two years or more post-surgery in a significant proportion of patients — even in those who have returned to sport and consider their rehabilitation complete. The deficit is not simply a matter of effort. It reflects a complex and sustained neurophysiological disruption that requires systematic rehabilitation to reverse.
The Inhibition-atrophy Cycle
After ACL injury, a self-reinforcing cycle commonly develops. Swelling and joint pathology create arthrogenic muscle inhibition, which reduces quadriceps activation. Reduced activation leads to disuse atrophy. As atrophy progresses, the capacity for voluntary activation further diminishes, and the inhibitory signals from the joint are more easily able to suppress what voluntary drive remains. Breaking this cycle requires two things simultaneously: reducing the joint pathology that drives inhibition, and providing sufficient neuromuscular stimulus to prevent or reverse the atrophic response. Neither alone is sufficient.
Why Gym Strength Does Not Always Reflect Functional Capacity
One of the most clinically significant findings in contemporary ACL rehabilitation research is the recognition that strength measured in the gym does not always accurately predict functional capacity during sport-specific tasks.
Lee Herrington’s research on neuromuscular control and limb symmetry in ACL rehabilitation has demonstrated that athletes who achieve acceptable quadriceps force production during slow, controlled gym-based assessment can simultaneously demonstrate significant deficits in dynamic loading tasks — landing mechanics, deceleration control, and single-leg force absorption — that require the quadriceps to produce and control force rapidly under conditions of instability.
Tom Goom (The Running Physio) has similarly emphasised that the ability to demonstrate adequate strength in a controlled gym environment does not confirm tissue readiness for the repetitive, cumulative loading demands of running. The distinction between isolated strength capacity and dynamic load tolerance maps directly onto the quadriceps challenge in ACL rehabilitation.
What LSI testing tells you — and where it falls short
The limb symmetry index compares performance between limbs but cannot account for whether the non-operated limb is itself at full capacity. A patient achieving 90% LSI may be comparing an inhibited post-operative limb to a somewhat deconditioned reference limb — potentially overestimating functional capacity.
Restoring Quadriceps Function: A Staged Rehabilitation Approach
Effective quadriceps restoration requires a staged approach progressing from addressing the neurological inhibition driving the initial deficit, through rebuilding fundamental strength, toward developing the dynamic force production and neuromuscular control that sport ultimately demands.
Stage 1: Reducing Inhibition
Weeks 0 — 4: Swelling management, early activation, and neuromuscular re-education
The priority is not strength — it is restoring the nervous system’s willingness to drive the quadriceps. This requires active swelling management alongside specific neuromuscular activation techniques including isometric contractions, neuromuscular electrical stimulation where appropriate, terminal knee extensions, and carefully dosed early loading. Rehabilitation at this stage should stimulate activation without provoking further joint irritability.
Stage 2: Building Strength Foundations
Weeks 4 — 10: Progressive loading, bilateral to unilateral, gym-based strengthening
As inhibition reduces, rehabilitation progressively introduces more structured loading. Heavy slow resistance principles — controlled tempo, progressive overload, sufficient volume — drive hypertrophy and motor unit recruitment. The transition from bilateral to unilateral loading is critical, introducing the single-leg demands that running and sport require. Blood flow restriction training has an important role during this stage, particularly where conventional loading remains restricted.
Stage 3: Developing Dynamic Capacity
Weeks 10+: Plyometric preparation, force absorption, and sport-specific loading
Adequate gym-based strength is a prerequisite for this stage, not a guarantee of readiness for it. The transition from heavy slow resistance work to plyometric and dynamic loading requires systematic progression through force absorption drills, landing mechanics work, hop preparation, and eventually higher-speed, higher-demand movements. The quadriceps must be able to produce force rapidly and eccentrically under dynamic conditions.
Blood Flow Restriction Training and Hytro BFR
Blood flow restriction training has become one of the most clinically important tools in ACL rehabilitation — particularly in the early post-operative period when heavy loading of the knee is either inappropriate or poorly tolerated due to pain, swelling, and tissue vulnerability.
BFR works by applying partial restriction to venous blood flow from the limb during resistance exercise. The resulting metabolic environment — lactate accumulation, cellular swelling, and hypoxic stress — creates a stimulus for muscle protein synthesis and motor unit recruitment that is normally associated with high-load training, at a fraction of the mechanical load. For post-operative patients who cannot yet tolerate conventional loading, this provides a clinically significant opportunity to maintain or rebuild muscle mass while healing tissue is protected.
Ramsey et al. (2021), in a systematic review and meta-analysis in Physical Therapy in Sport, demonstrated that BFR training in the early post-operative period following ACL reconstruction significantly attenuated quadriceps atrophy and reduced limb symmetry index deficits compared to conventional low-load training alone. The effect was most pronounced in the first eight to twelve weeks post-surgery — precisely the window when conventional loading is most restricted.
Active BFR: During Exercise
Active BFR involves wearing a graduated compression garment or cuff during resistance exercise sessions. At Atherapy, we integrate Hytro BFR shorts and upper garments into the rehabilitation programme where clinically appropriate, allowing patients to perform their exercise programme — squats, leg press, step-up work, cycling — under controlled blood flow restriction. This maximises the neuromuscular and hypertrophic stimulus from each session, even at loads that would otherwise be insufficient to drive meaningful adaptation.
Active BFR is particularly valuable during phases two and three of quadriceps rehabilitation, where the goal is progressive loading but conventional heavy resistance work may still be constrained by tissue tolerance, swelling response, or graft protection requirements.
Passive BFR: Between Sessions
Passive BFR involves wearing compression garments at rest or during low-intensity activity — not during exercise itself. The mechanism is distinct from active BFR: passive restriction during rest creates a mild hypoxic environment within the muscle that stimulates protein synthesis pathways and may attenuate the disuse atrophy that develops rapidly during periods of enforced unloading.
In the immediate post-operative period — when patients are weight-bearing with crutches, sleeping, travelling, or simply resting — passive BFR garments offer a low-demand way to maintain some protective stimulus to the quadriceps during the hours between clinical sessions. For patients who are significantly limited in what they can do actively in the first weeks after surgery, this represents a meaningful addition to the rehabilitation toolkit.
At Atherapy, we use Hytro BFR garments in both active and passive applications as part of our quadriceps rehabilitation programme, guided by individual clinical assessment and tolerance.
BFR contraindications and clinical considerations
Blood flow restriction training is not appropriate for all patients. Contraindications include deep vein thrombosis or significant risk of DVT, significant cardiovascular or vascular disease, sickle cell anaemia, compromised wound healing at the garment application site, and certain clotting disorders. BFR should always be assessed for clinical appropriateness before use and applied under clinical supervision with appropriate equipment and pressure calibration. At Atherapy, BFR — including Hytro garments — is used selectively as part of a broader, individually assessed quadriceps rehabilitation programme.
Bridging The Gap: From Gym Strength To Dynamic Performance
Perhaps the most clinically important phase of quadriceps rehabilitation is the transition from demonstrating adequate gym-based strength to expressing that strength under dynamic, sport-relevant conditions.
A patient may achieve a satisfactory limb symmetry index while simultaneously demonstrating significant landing asymmetry during hop testing, reduced knee flexion during running, and protective movement strategies during deceleration. These discrepancies reflect that isolated strength and dynamic neuromuscular control are related but distinct capacities that require different rehabilitation stimuli to develop.
As Tom Goom (The Running Physio) has emphasised in his work on rehabilitation load management, the capacity to tolerate running demands is not simply a function of having adequate strength in isolation — it requires the progressive, repeated exposure of the neuromuscular system to the specific loading patterns that running creates. Strength is the foundation. Dynamic capacity is the structure built on it.
At Atherapy, bridging this gap involves systematic progression through landing mechanics work, single-leg hop preparation, eccentric loading under dynamic conditions, deceleration drills, and sport-specific movement exposure — all calibrated to the individual’s current quadriceps capacity and the specific demands of their sport.
Quadriceps Weakness and Reinjury Risk
Grindem et al. (2016) demonstrated in the Delaware-Oslo cohort that athletes returning to pivoting sport with a quadriceps limb symmetry index below 90% were at dramatically elevated risk of second injury — and that meeting simple objective criteria including quadriceps symmetry reduced reinjury risk by up to 84%. Lee Herrington’s work on neuromuscular deficits and landing mechanics has further demonstrated that residual quadriceps weakness creates the altered landing strategies and reduced deceleration control that place the reconstructed knee in higher-risk positions during cutting and pivoting movements.
Returning to sport before restoring adequate quadriceps function is not simply suboptimal rehabilitation. It is a meaningful and largely preventable elevation in injury risk. Objective testing of quadriceps strength before return to sport is therefore not bureaucratic caution — it is basic clinical responsibility.
Speak To A Clinician About Your ACL Prehabilitation Programme
If you have recently sustained an ACL injury, are awaiting surgical opinion, or want expert guidance on preparing for reconstruction, our clinical team will design a structured programme tailored to your injury, sport, surgical pathway, and long-term performance goals.
Evidence & Research References
This page reflects current evidence-based practice in quadriceps rehabilitation following ACL injury and reconstruction. Key research informing the content includes:
- Rice DA, McNair PJ (2014). Quadriceps arthrogenic muscle inhibition: neural mechanisms and treatment perspectives. Seminars in Arthritis and Rheumatism.
- Lepley LK et al. (2017). Quadriceps strength deficits persist two years after ACL reconstruction. Journal of Athletic Training.
- Grindem H et al. (2016). Simple decision rules can reduce reinjury risk by 84% after ACL reconstruction. British Journal of Sports Medicine.
- Buckthorpe M et al. (2021). Recommendations for assessment and progressive return to sport after lower limb muscle injury. Sports Medicine.
- Ramsey P et al. (2021). Blood flow restriction training in the rehabilitation of anterior cruciate ligament injuries: a systematic review. Physical Therapy in Sport.
- Kotsifaki A et al. (2022). Single leg vertical jump performance identifies knee function deficits at return to sport after ACL reconstruction. British Journal of Sports Medicine.
- Losciale JM et al. (2022). The association between passing return-to-sport criteria and second ACL injury risk. British Journal of Sports Medicine.
Clinical frameworks informing this page include the work of Mick Hughes (ACL rehabilitation criterion-based frameworks and quadriceps restoration protocols), Lee Herrington (neuromuscular control deficits and limb symmetry assessment in ACL rehabilitation), and Tom Goom, The Running Physio (load management principles and the quadriceps-to-running progression).
Melbourne ACL Rehabilitation Guide and Aspetar Return-to-Sport Guidelines also inform this content. Rehabilitation should always remain individualised.
London Physiotherapy Team
Welcome to the Atherapy expert clinical team. We are a dedicated group of qualified physiotherapists and sports medicine specialists committed to delivering innovative, evidence-based rehabilitation. Our practice is built on a holistic approach to physical health, firmly believing that injury prevention is just as vital as the cure. From treating acute sports injuries to designing custom performance optimization programs, our clinicians work collaboratively to help you safely reach your goals.
Meet our resident experts below and find the right specialist for your recovery journey.

- With 25+ years of Premier League and Championship experience, Andrew has led Medical, Science, and Performance departments for Hull City, Nottingham Forest, Derby County, and Preston North End, following earlier work at the Manchester United Academy
- Specialist in lower limb rehabilitation
- Post-operative rehabilitation
- Back pain and complex spinal presentations
- Elite athlete management including manual therapy, gym rehabilitation and acupuncture
- Specialises in complex cases and second opinion rehabilitation planning including return to play
- Limited clinical availability due to wider clinical leadership and operational responsibilities
Andrew Balderston
Based at Moorgate

- Specialist in exercise-based rehabilitation, manual therapy and injury prevention
- Experienced in post-operative rehabilitation and progressive return to activity
- Clinical interests include sports injuries, cervical spine and low back dysfunction, shoulder, knee, foot and ankle rehabilitation
- Combines hands-on treatment with targeted strength and rehabilitation programming
- Focused on structured rehabilitation to help patients rebuild strength, movement confidence and function
- Specialist interest in women’s health support including manual lymphatic drainage during pregnancy and pre/post-natal care
- Over 15 years of clinical experience across private practice, sports rehabilitation and women’s health settings
- Fluent in English, Portuguese and Italian
Fernanda Saldanha
Based at Chiswick

- Extensive experience working within elite professional football and private practice
- Former Tottenham Hotspur Academy physiotherapist specialising in performance rehabilitation and return-to-play management
- Specialist interest in post-operative rehabilitation and upper and lower limb injury management
- Experienced in managing complex and recurrent injuries through structured, evidence-based rehabilitation planning
- Clinical approach combines manual therapy, gym-based rehabilitation, movement analysis and acupuncture
- Focused on restoring movement quality, strength under load and long-term performance outcomes
- Fluent in English and Greek
Dimitrios Michtatidis
Based at Chiswick and Strand

- Level 4 Strength & Conditioning Coach
- Medical Acupuncture & Dry Needling Qualified
- Combines detailed clinical assessment with progressive rehabilitation and strength & conditioning principles
- Specialist interest in gym-based rehabilitation and return-to-sport management
- Clinical interests include acute sporting injuries, post-operative orthopaedic rehabilitation (including ligament reconstructions, meniscal and labral repairs) and hip/groin pain in active populations
- Experience managing both active general population and performance-focused clients
- Adjunct treatment techniques include dry needling and shockwave therapy
Claire Cuffe
Based at Moorgate and Strand

- Over 5 years experience treating orthopaedic injuries, chronic pain and post operative care
- Advanced certifications in dry needling for hands, face, feet, lower limb, upper limb and lumbopelvic region
- Certified pelvic floor physio for both men and women with an interest in treating clients pre and post natal
- Special interest in strength and conditioning programming for clients training for half/full marathons




