

ACL Rehabilitation
Meniscal Injury Alongside ACL Reconstruction: What It Means for Your Rehabilitation
When patients receive their post-operative surgical notes, one phrase appears with striking regularity alongside the ACL reconstruction: concomitant meniscal tear. For many patients this arrives as a surprise - they came in for an ACL injury and emerge from theatre to learn they also had meniscal surgery. What was done to the meniscus, and why, is often inadequately explained in the immediate post-operative period. The consequences for rehabilitation are significant and specific.
Meniscal injury alongside ACL rupture is not the exception - it is the rule. Norwegian Knee Ligament Registry data from 5,309 ACLR knees identified that 68% had one or more recorded meniscal injuries (Stensrud et al., 2025). At Atherapy, understanding what the surgeon did to the meniscus is as important as knowing the ACL graft type. The two decisions together determine the rehabilitation programme that follows.
How Common Is Meniscal Injury With ACL Rupture
The co-occurrence of meniscal injury with ACL rupture reflects the shared mechanism of injury. The twisting, deceleration, and pivoting forces that rupture the ACL simultaneously load the menisci beyond their tolerance in the majority of cases. Medial meniscal tears are more common in chronic ACL-deficient knees - the meniscus gradually takes on increased load as the absent ACL allows anterior tibial translation. Lateral meniscal tears are more common in acute ACL injuries, particularly the lateral meniscus posterior root tear (LMPRT) and ramp lesion, which occur at the point of injury rather than developing over time.
Norwegian registry data identifies LMPRTs in 10% and ramp lesions in 7.8% of primary ACLRs - both significantly under diagnosed in standard operative reporting. Winter sports showed the highest sport-specific incidence of both injury types at 14%. The clinical implication is that any patient presenting with ACL rupture should have explicit discussion with their surgical team about meniscal involvement, and any rehabilitation programme should begin by establishing precisely what was found and treated.
A further finding with direct clinical relevance is the relationship between delay to surgery and meniscal injury severity. Lu and colleagues (AJSM, 2022) used machine learning survival analysis on a Mayo Clinic dataset to show that early ACL reconstruction significantly reduces the risk and delays the timing of secondary meniscal injury compared to delayed reconstruction or non-operative management. Gupta and colleagues (Orthopaedic Journal of Sports Medicine, 2023) found that among 542 patients who had MRI within three weeks of injury, delayed ACLR of eight weeks or more was associated with a 3.9-fold higher risk of new medial meniscal tears in paediatric patients and a substantially higher new lateral meniscal tear rate in adults. The message is clear: a knee with an intact ACL graft provides a mechanically protective environment for the menisci; an ACL-deficient knee that continues to experience episodes of instability progressively damages the meniscal tissue that the reconstruction will need to protect.
The Meniscus and Why It Matters
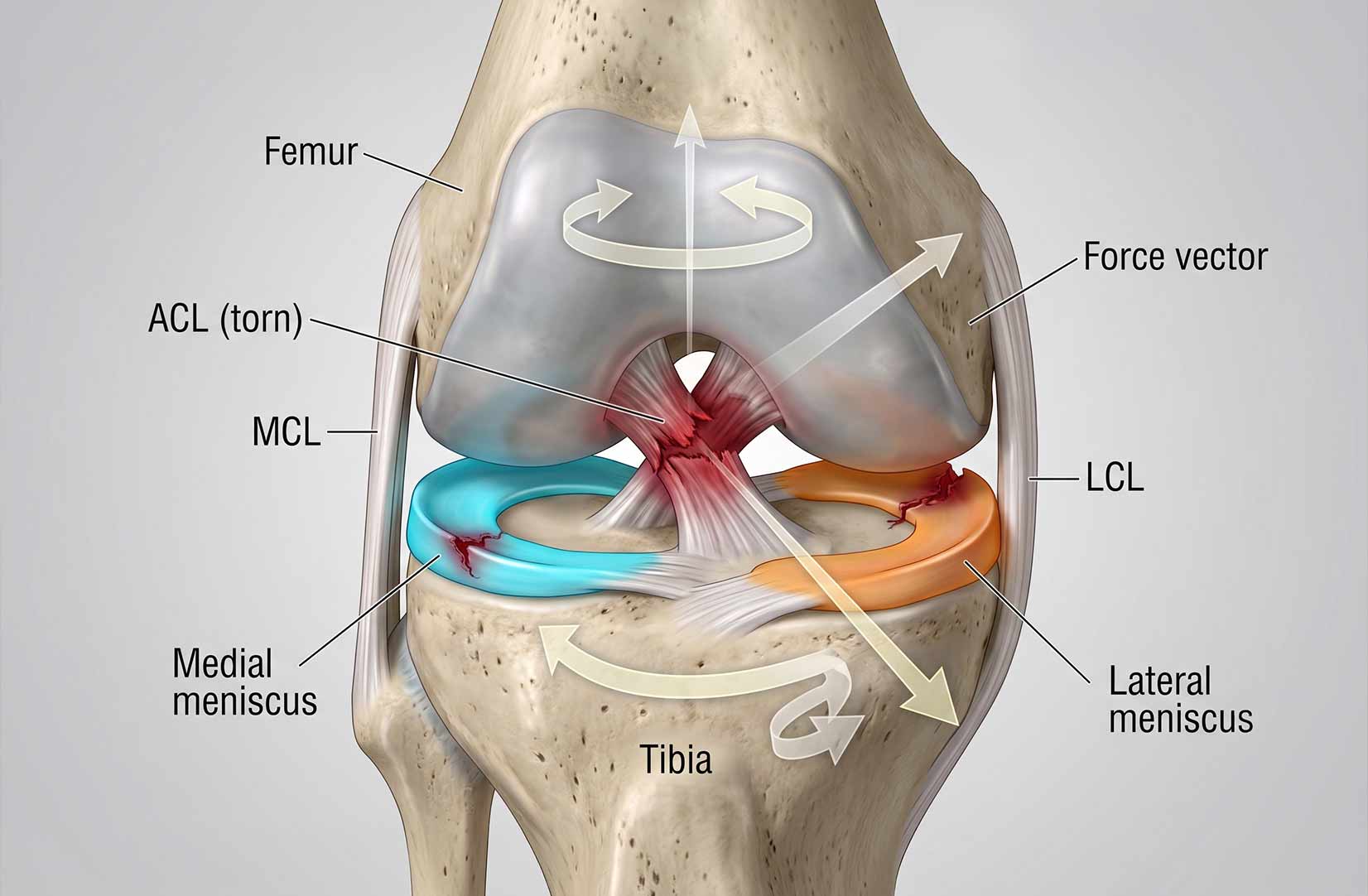
The menisci are two C-shaped fibrocartilaginous structures that sit between the femur and tibia - the medial meniscus on the inner side of the knee, the lateral meniscus on the outer side. They perform multiple functions that are central to long-term knee health: load distribution across the joint surface (absorbing approximately 50-70% of compressive load in extension and up to 85% in flexion), shock absorption, joint lubrication, secondary restraint to anterior tibial translation, and joint stability through their conforming effect on the articular surfaces.
The loss of meniscal tissue through partial meniscectomy concentrates joint load onto the articular cartilage, accelerating wear. This is the fundamental basis for the well-established link between meniscectomy and osteoarthritis. The extent of that risk depends on which meniscus is removed, how much is removed, and what the mechanical environment of the knee looks like over subsequent decades. It is also the fundamental reason why the surgical philosophy over the past two decades has shifted decisively toward meniscal preservation and repair over resection wherever the biology supports it.
"The meniscus is not just a cushion. It is a load distributor, a shock absorber, a stability structure, and a joint protector. Its preservation or loss has consequences that extend decades beyond the rehabilitation period."
Repair vs Resection: Two Very Different Rehabilitation Paths
The surgical decision at the time of ACL reconstruction - whether to repair the meniscus, resect the damaged portion, or leave it in situ - has a more immediate and specific impact on rehabilitation than almost any other intra-operative finding. The two main options create fundamentally different post-operative environments.
Meniscal repair preserves the tissue and aims to restore its function, but the repair must be protected during the healing period. The repaired meniscal tissue is vulnerable to compressive and shear forces during the first 6 to 12 weeks post-operatively, and excessive loading during this window risks repair failure. This necessitates weight-bearing and range of motion restrictions that have direct consequences for the ACL rehabilitation programme running in parallel. Partial meniscectomy removes the damaged tissue and eliminates the immediate protection concern, allowing a rehabilitation protocol driven entirely by the ACL reconstruction requirements. The trade-off is long-term: removing meniscal tissue increases joint load on the articular cartilage and, in the medial compartment particularly, elevates osteoarthritis risk.
Meniscal Repair: The Modified Rehabilitation Protocol
The 2024 EU-US Meniscus Rehabilitation Consensus - a combined ESSKA-AOSSM-AASPT initiative involving 67 experts from 14 countries - is now the most authoritative international guidance on post-operative meniscal management and supersedes previous patchwork of individual surgeon protocols. Its key recommendations for repair rehabilitation are tear-type specific rather than universally restrictive.
For stable vertical tears where the hoop fibre integrity is preserved, an accelerated protocol is supported: partial weight-bearing of approximately 20kg for the first four weeks, with range of motion limited to 90 degrees, progressing to full weight-bearing thereafter. For complex tears - horizontal, radial, and root repairs where hoop fibres are disrupted - a restricted protocol is recommended: non-weight-bearing for the first six weeks with ROM limited to 90 degrees. The distinction matters because applying a universal restrictive protocol to all repair patients imposes unnecessary constraints and delays, while applying an accelerated protocol to complex repairs risks the integrity of the repair. A 2025 systematic review by Bouchard and colleagues (Orthopaedic Journal of Sports Medicine, 2025) — covering 10 studies and 313 patients through November 2024 — found that accelerated weight-bearing protocols were used in 7 of 10 studies with low failure rates, providing evidence that the universal non-weight-bearing approach is not necessary for stable peripheral repairs when patient and tear selection is appropriate.
Where meniscal repair is performed simultaneously with ACL reconstruction, the EU-US Consensus confirms that rehabilitation protocols are similar to isolated meniscal repair, but return to sport may be further delayed on account of the ACL reconstruction running in parallel. Crucially: the more restrictive protocol governs. If the meniscal repair requires non-weight-bearing for 6 weeks, that restriction takes precedence over the ACL rehabilitation weight-bearing progression, regardless of how the ACL is recovering. This is the most common source of confusion in combined post-operative rehabilitation - patients and some non-specialist physiotherapists proceed with ACL weight-bearing milestones without appreciating that the meniscal repair imposes stricter constraints.
Partial Meniscectomy: When the Protocol Differs Less Than Expected
Partial meniscectomy - arthroscopic removal of the damaged meniscal tissue while preserving the remaining healthy meniscus - creates a simpler immediate post-operative environment than repair. The EU-US Consensus is clear: following partial meniscectomy, immediate full weight-bearing and full range of motion are permitted as tolerated per symptoms (Grade A evidence). No weight-bearing restriction is required. No ROM restriction is imposed. The rehabilitation programme is governed by the ACL reconstruction requirements, not the meniscal procedure.
This is counterintuitive to many patients who assume meniscal surgery automatically means extended restrictions. In practice, a patient who has had partial meniscectomy alongside ACL reconstruction may experience marginally more early post-operative swelling and may need slightly longer to achieve comfortable full extension under load, but their rehabilitation trajectory follows the standard ACL programme without meniscal-specific modification.
The long-term concern with partial meniscectomy is different from the short-term picture. Swedish National Knee Ligament Registry data tracking over 22,000 patients found that medial meniscal resection is associated with accelerated articular cartilage deterioration over 5 to 10 years. Lateral meniscectomy showed no significant increase in cartilage injury risk at 10-year follow-up in the same dataset - a nuance in the evidence that has implications for how long-term loading and return-to-sport decisions are framed in medial versus lateral meniscectomy cases. For patients with medial meniscal resection, the rehabilitation and post-return conditioning programme should incorporate load management principles that reflect the reduced shock-absorbing capacity of the compartment.
The Third Option: Leaving the Tear In Situ
A surgical decision that patients rarely have explained to them is the option to leave a meniscal tear untreated at the time of ACL reconstruction - neither repairing nor resecting it. This is sometimes described in operative notes as "left in situ" or "observed." It is a recognised clinical decision applied to tears that are considered stable, small, or located in regions with limited blood supply where repair is unlikely to succeed and where the tear itself is not causing mechanical symptoms.
The Swedish National Knee Ligament Registry data from Stenlund and colleagues provides the most important evidence on this decision. Analysing over 22,000 patients, they found that leaving lateral meniscal tears in situ was associated with significantly higher odds of revision ACL reconstruction at both five years (odds ratio 1.49) and ten years (odds ratio 1.55) compared to isolated ACLR. This finding challenges the assumption that ignoring a stable-looking tear at the time of reconstruction is a low-risk default. The unstable knee environment prior to reconstruction may have created a tear pattern that appears stable but continues to generate symptoms or instability post-operatively.
The clinical implication for rehabilitation is less about protocol modification and more about surveillance and communication. A patient whose operative notes specify that a meniscal tear was left in situ should understand that this does not mean the tear has resolved - it means the surgeon made a judgement that it did not require treatment at that time. Any recurrence of mechanical symptoms (clicking, locking, specific pain patterns distinct from the ACL recovery) in the weeks following surgery warrants prompt reporting and assessment rather than assuming it is part of standard post-operative recovery.
Ramp Lesions and Root Tears: The Injuries Surgeons Are Increasingly Treating
Two specific meniscal injury patterns deserve particular attention because they are increasingly identified and treated at primary ACL reconstruction, yet are poorly understood by most patients.
Ramp Lesions
A ramp lesion is a peripheral tear of the posterior horn of the medial meniscus at the meniscocapsular junction - the interface between the meniscus and the posterior joint capsule. They are identified in 7.8% of primary ACLRs in registry data but are frequently missed on pre-operative MRI and only diagnosed during arthroscopy when the posterior compartment is specifically examined.
Ramp lesions are clinically significant because they compromise the meniscus as a secondary restraint to anterior tibial translation. An unrepaired ramp lesion in an ACL-reconstructed knee leaves the graft exposed to higher loads than in a knee with an intact posterior horn - potentially contributing to graft failure risk.
Rehabilitation implication: ramp lesion repair typically follows a similar protocol to other peripheral meniscal repairs. ROM and weight-bearing restrictions apply per the surgeon protocol, and deep knee flexion is restricted in the early post-operative phase. Confirm with the operative notes whether the ramp lesion was repaired, left in situ, or treated differently.
Lateral Meniscus Posterior Root Tears (LMPRTs)
The lateral meniscus posterior root is the attachment point where the posterior horn of the lateral meniscus anchors to the tibia. A LMPRT at the time of ACL injury effectively unlocks the meniscus from its tibial anchor, rendering it unable to function as a hoop - the circumferential tension mechanism that distributes compressive load.
Found in 10% of primary ACLRs in registry data, LMPRTs are associated with older patients and are more common in non-contact injury mechanisms. Incidence reaches 15-31% in some series, and is four times higher on the lateral than medial side at the time of primary ACLR.
Rehabilitation implication: LMPRT repair requires the most conservative weight-bearing protocol of any concomitant meniscal procedure. Non-weight-bearing for 6 weeks is standard, progressing to full weight-bearing by 8 weeks. Weight-bearing through a flexed knee - stairs, squatting, lunging - is delayed beyond this period. Root repairs have the highest failure risk of any meniscal repair type and require the most diligent adherence to restrictions.
What the Outcome Data Shows
The most current registry-level evidence on concomitant meniscal surgery with ACLR presents a nuanced picture that should inform patient counselling before rehabilitation begins. The UK National Ligament Registry study (2024), analysing over nine years of prospectively collected data, found that medial meniscal repair combined with ACLR was associated with inferior patient-reported outcome measures at two years compared to isolated ACLR - a statistically significant difference that nonetheless resolved by five years, with no meaningful difference in outcomes between groups at that point. The message: meniscal repair patients should expect a slower early trajectory without interpreting it as failure.
For professional athletes specifically, the SANTI Study Group data is the most relevant published series. An and colleagues (Orthopaedic Journal of Sports Medicine, 2025) analysed 196 professional athletes at the Centre Orthopaedique Santy - a FIFA Medical Centre of Excellence - over a mean follow-up of 96 months. They found that 85.2% of professional athletes had meniscal lesions at the time of ACL reconstruction. At long-term follow-up, the overall meniscal repair failure rate was 13.2% - 5% for lateral meniscal repairs and 15.4% for medial meniscal repairs. No risk factors for secondary meniscectomy were identified, underscoring how difficult it remains to predict which individual repairs will fail. This is the most directly football-relevant failure data in the current literature, and it contextualises the repair versus resection decision in a way that resonates with players and their teams.
Return to sport is the outcome most patients prioritise, and here the MERIscience cohort study (Orthopaedic Journal of Sports Medicine, 2025) adds an important new dimension. Analysing five-year follow-up data from patients who underwent hamstring autograft ACLR with or without meniscal procedures, the study found that medial meniscal injury at the time of ACLR was associated with significantly lower return-to-sport rates and poorer patient-reported outcomes. The clinical message is precise: medial meniscal involvement is not just a technical complication of the reconstruction - it is an independent predictor of longer-term functional recovery and return-to-sport success. Identifying and repairing medial meniscal tears wherever possible, the authors concluded, is an important strategy for improving outcomes in patients undergoing ACLR.
The evidence on repair versus resection has also sharpened. Swedish National Knee Ligament Registry data from Stenlund and colleagues, analysing patients with concurrent lateral meniscal injury, found that lateral meniscal repair was associated with higher odds of revision ACLR at five years than resection in that cohort — a counterintuitive finding that has generated debate and reflects the complexity of tear pattern selection for repair. The Perraut et al. (2024) data on bucket-handle meniscal tears is more straightforward: repair produced significantly better patient-reported outcomes than partial meniscectomy in this tear pattern, supporting the established principle that when the tissue is reparable, repair produces better long-term outcomes.
For footballers specifically, Moretti and colleagues (Orthopaedic Journal of Sports Medicine, 2023) studied 51 male soccer players who had undergone ACLR with or without concomitant meniscal repair, finding that biomechanical performance measures and fear of reinjury were significantly worse in players with associated meniscal repair at minimum 1-year follow-up — particularly those with lateral meniscal repair, who showed lower strength symmetry, balance, and coordination alongside higher pain and fear of reinjury scores. This is an important finding for clinical counselling: it means that for footballers, meniscal repair extends not just the formal rehabilitation period but the functional reintegration timeline, and return-to-full-performance expectations should be set accordingly.
Across all the evidence, a consistent theme emerges: the worse short-term outcomes associated with meniscal repair reflect the constraints it imposes on rehabilitation, not the inadequacy of the procedure itself. By five years, outcomes converge or favour repair in most series. The rehabilitation job is to navigate the constraints of the repair period competently, maintain muscle mass and neuromuscular control within the limits imposed, and build progressively toward full function once those constraints are lifted.
Strength, Atrophy and the Restricted Phase: What the Evidence Shows
A question patients frequently ask — and one that deserves a direct answer — is whether having meniscal repair leaves a lasting strength deficit beyond the ACL reconstruction itself. The evidence on this is more reassuring than the restrictions might suggest. Wenning and colleagues (Archives of Orthopaedic and Trauma Surgery, 2020) compared isokinetic strength recovery at 6 months post-surgery between isolated ACLR, ACLR with meniscal repair, and ACLR with meniscectomy, and found that concomitant meniscal repair did not significantly compound the quadriceps strength deficit compared to ACLR alone at return-to-sport stage. Mesnard and colleagues at the FIFA Medical Centre of Excellence in Lyon (SICOT-J, 2022) reported the same finding in a cohort of patients assessed with isokinetic testing. The EU-US Consensus reinforces this: it recommends quadriceps strength testing at each phase of rehabilitation using isokinetic or handheld dynamometry, and does not classify meniscal repair as an independent predictor of worse long-term strength outcomes.
The important qualification is timing. The MERIscience group published a 504-patient analysis (Cazemajou et al., Journal of Clinical Medicine, 2024) showing that associated medial meniscal injury with ACLR produces significantly poorer strength and jump test outcomes at 6 months — the period that directly overlaps with the weight-bearing restricted phase for many repair patients. The deficit at 6 months is real and clinically significant. The evidence suggests it resolves by return-to-sport stage in most patients who follow an appropriately structured programme. The rehabilitation task is to manage the restricted phase intelligently so that the 6-month snapshot does not become a long-term trajectory.
Blood Flow Restriction Training in Meniscal Repair Rehabilitation
Blood flow restriction (BFR) training has a particularly valuable role in meniscal repair rehabilitation that goes beyond its standard application in ACL recovery. The weight-bearing and range of motion restrictions imposed by complex meniscal repairs create a period of enforced relative immobilisation that significantly elevates atrophy risk. During this window, conventional strength training is not possible — loading the repaired tissue is precisely what must be avoided. BFR training addresses this by producing meaningful muscle hypertrophy and strength stimulus at very low mechanical loads, restricting venous blood return during exercise to create metabolic stress sufficient to drive adaptation without requiring the joint loading that would jeopardise the repair.
The application of BFR during the restricted phase is supported by published clinical guidance. For patients where full quadriceps loading is not possible, isometric quadriceps exercises and very low load isotonic work with BFR can meaningfully attenuate the atrophy that otherwise accumulates during weeks two through six post-operatively — the period when the MERIscience data shows the greatest strength divergence between meniscal and non-meniscal repair groups. The Hytro BFR garment — which allows passive BFR to be worn at rest as well as during active exercise — has a specific role here: passive BFR worn during periods of rest or restricted activity produces a metabolic environment that further reduces atrophy compared to rest alone.
What Meniscal Injury Means at Atherapy
At Atherapy, the first question asked of any post-operative ACL patient is not how they feel, but what the operative notes say. Graft type, meniscal treatment, concurrent procedures, and surgeon-specified restrictions are all established before rehabilitation begins. For patients with meniscal repair, the surgeon protocol is obtained and followed precisely - the EU-US Consensus recommendations are used as a framework, but individual surgeon protocols take precedence where they are more conservative.
Patients with meniscal repair are counselled explicitly from the first session about what the modified timeline means, why it exists, and what the outcome data shows. The message is consistent with the UK National Ligament Registry evidence: the slower early trajectory is a feature of repair, not a complication. By five years, outcomes converge with those of patients without meniscal involvement. The job of rehabilitation is to protect the repair during its critical healing window, maintain as much strength and neuromuscular control as the restrictions permit, and build competently toward full load once those restrictions are lifted.
Game Ready cold-compression therapy is particularly valuable in the early post-operative period for meniscal repair patients, where swelling management directly affects arthrogenic muscle inhibition and rehabilitation progress during the restricted weight-bearing phase.
Repair vs Resection - Rehabilitation Comparison
Summary of key rehabilitation differences by surgical decision:
Related Pages in the ACL Rehabilitation Series
→ Post-Operative ACL Rehabilitation
→ Quadriceps Weakness After ACL Injury
→ Swelling After ACL Reconstruction
→ Reinjury Risk After ACL Surgery
Rehabilitation After ACL Reconstruction With Meniscal Surgery - Atherapy
If you have had ACL reconstruction with concurrent meniscal surgery - repair or resection - your rehabilitation programme needs to be built around both procedures, not just the ACL. At Atherapy, we begin with your operative notes and build a programme that reflects exactly what was done, what restrictions apply, and what timeline is realistic given the evidence. Bring your surgical discharge summary to your first appointment.
References
- Stensrud S, et al. Incidence and treatment strategy of lateral meniscus posterior root tears and ramp lesions identified during isolated ACL reconstructions: report from a nationwide knee ligament register. American Journal of Sports Medicine. 2025;53(7). doi:10.1177/03635465251417254.
- Formal EU-US Meniscus Rehabilitation 2024 Consensus - An ESSKA-AOSSM-AASPT Initiative. Part I: Rehabilitation management after meniscus surgery (meniscectomy, repair and reconstruction). International Journal of Sports Physical Therapy / JOSPT Open. 2024. doi:10.26603/001c.137095.
- Calanna F, Duthon V, Menetrey J. Rehabilitation and return to sports after isolated meniscal repairs: a new evidence-based protocol. Journal of Experimental Orthopaedics. 2022;9(1):87.
- UK National Ligament Registry. The impact of concomitant meniscal surgery on the clinical outcomes of anterior cruciate ligament reconstruction. Bone and Joint Open. 2024;5(11):1003-1012.
- Stenlund P, et al. Long-term effects of concomitant lateral meniscal management on ACL reconstruction revision rate and secondary meniscal and cartilaginous injuries. American Journal of Sports Medicine. 2025. PMC12056325.
- Perraut GT, Cherelstein RE, Galel AM, et al. Repair of bucket handle meniscus tears improves patient outcomes versus partial meniscectomy at the time of ACL reconstruction. Journal of Experimental Orthopaedics. 2024;11(4):e70004.
- Brinkman JC, Tummala SV, Parmar R, et al. High failure rate in meniscal repair when preceding anterior cruciate ligament reconstruction: an analysis of two-stage surgery for concomitant ACL injury and traumatic meniscus tear. Knee Surgery, Sports Traumatology, Arthroscopy. 2025. doi:10.1002/ksa.12755.
- An JS, Lahsika M, Nlandu A, et al. Failure rate of meniscal repair with ACL reconstruction among professional athletes: a study of 196 patients from the SANTI Study Group with a mean follow-up of 96 months. Orthopaedic Journal of Sports Medicine. 2025;13(2):23259671241308591. [Centre Orthopaedique Santy, FIFA Medical Centre of Excellence]
- MERIscience cohort. Association between meniscal injuries at the time of an anterior cruciate ligament reconstruction and lower return-to-sport rates: an analysis at 5 years of follow-up. Orthopaedic Journal of Sports Medicine. 2025. PMC12413527.
- Lu Y, Jurgensmeier K, Till SE, et al. Early ACL reconstruction and risk and timing of secondary meniscal injury compared with delayed ACLR or nonoperative treatment: a time-to-event analysis using machine learning. American Journal of Sports Medicine. 2022;50(13):3544-3556.
- Gupta A, Badin D, Ortiz-Babilonia C, Davidson AJ, Lee RJ. Is delayed anterior cruciate ligament reconstruction associated with a risk of new meniscal tears? Reevaluating a longstanding paradigm. Orthopaedic Journal of Sports Medicine. 2023;11(10):23259671231203239.
- Bouchard MD, Macciacchera M, Gilbert J, Lameire DL, Abouali J. Postoperative rehabilitation protocol after isolated meniscal repair: a systematic review. Orthopaedic Journal of Sports Medicine. 2025;13(7):23259671251357513.
- Cazemajou C, Marty-Diloy T, Graveleau N, Laboudie P, Bouguennec N. Associated medial meniscal injury with ACL reconstruction results in poorer strength and jump tests outcomes: a 6-month analysis of 504 patients from the MERIScience cohort. Journal of Clinical Medicine. 2024;13(23):7251.
- Moretti L, Bortone I, Delmedico M, et al. Clinical, biomechanical, and self-reported health status after ACL reconstruction with meniscal repair in soccer players: results at minimum 1-year follow-up. Orthopaedic Journal of Sports Medicine. 2023;11(8):23259671231177309.
- Mesnard G, Fournier G, Joseph L, et al. Does meniscal repair impact muscle strength following ACL reconstruction? [FIFA Medical Centre of Excellence, Lyon]. SICOT-J. 2022;8:19.
- Wenning M, Heitner AH, Mauch M, et al. The effect of meniscal repair on strength deficits 6 months after ACL reconstruction. Archives of Orthopaedic and Trauma Surgery. 2020;140(9):1207-1215.
- Blood flow restriction training for meniscus repair surgery. Arthroscopy Techniques. 2025. PMC11997138.
- Kotsifaki R, Korakakis V, King E, et al. Aspetar clinical practice guideline on rehabilitation after anterior cruciate ligament reconstruction. British Journal of Sports Medicine. 2023;57(9):500-514.
London Physiotherapy Team
Welcome to the Atherapy expert clinical team. We are a dedicated group of qualified physiotherapists and sports medicine specialists committed to delivering innovative, evidence-based rehabilitation. Our practice is built on a holistic approach to physical health, firmly believing that injury prevention is just as vital as the cure. From treating acute sports injuries to designing custom performance optimization programs, our clinicians work collaboratively to help you safely reach your goals.
Meet our resident experts below and find the right specialist for your recovery journey.

- With 25+ years of Premier League and Championship experience, Andrew has led Medical, Science, and Performance departments for Hull City, Nottingham Forest, Derby County, and Preston North End, following earlier work at the Manchester United Academy
- Specialist in lower limb rehabilitation
- Post-operative rehabilitation
- Back pain and complex spinal presentations
- Elite athlete management including manual therapy, gym rehabilitation and acupuncture
- Specialises in complex cases and second opinion rehabilitation planning including return to play
- Limited clinical availability due to wider clinical leadership and operational responsibilities
Andrew Balderston
Based at Moorgate

- Specialist in exercise-based rehabilitation, manual therapy and injury prevention
- Experienced in post-operative rehabilitation and progressive return to activity
- Clinical interests include sports injuries, cervical spine and low back dysfunction, shoulder, knee, foot and ankle rehabilitation
- Combines hands-on treatment with targeted strength and rehabilitation programming
- Focused on structured rehabilitation to help patients rebuild strength, movement confidence and function
- Specialist interest in women’s health support including manual lymphatic drainage during pregnancy and pre/post-natal care
- Over 15 years of clinical experience across private practice, sports rehabilitation and women’s health settings
- Fluent in English, Portuguese and Italian
Fernanda Saldanha
Based at Chiswick

- Extensive experience working within elite professional football and private practice
- Former Tottenham Hotspur Academy physiotherapist specialising in performance rehabilitation and return-to-play management
- Specialist interest in post-operative rehabilitation and upper and lower limb injury management
- Experienced in managing complex and recurrent injuries through structured, evidence-based rehabilitation planning
- Clinical approach combines manual therapy, gym-based rehabilitation, movement analysis and acupuncture
- Focused on restoring movement quality, strength under load and long-term performance outcomes
- Fluent in English and Greek
Dimitrios Michtatidis
Based at Chiswick and Strand

- Level 4 Strength & Conditioning Coach
- Medical Acupuncture & Dry Needling Qualified
- Combines detailed clinical assessment with progressive rehabilitation and strength & conditioning principles
- Specialist interest in gym-based rehabilitation and return-to-sport management
- Clinical interests include acute sporting injuries, post-operative orthopaedic rehabilitation (including ligament reconstructions, meniscal and labral repairs) and hip/groin pain in active populations
- Experience managing both active general population and performance-focused clients
- Adjunct treatment techniques include dry needling and shockwave therapy
Claire Cuffe
Based at Moorgate and Strand

- Over 5 years experience treating orthopaedic injuries, chronic pain and post operative care
- Advanced certifications in dry needling for hands, face, feet, lower limb, upper limb and lumbopelvic region
- Certified pelvic floor physio for both men and women with an interest in treating clients pre and post natal
- Special interest in strength and conditioning programming for clients training for half/full marathons




